Chapters
Susan A. Bartels, Matthew M. Hall, Frederick M. Burkle Jr., and Gregg Greenough., Complex Emergencies, 9-2015, Ciottone?s Disaster Medicine, Vol. 2015, xx
M.L.A. Sivilotti, Initial Management of the critically ill adult with an unknown overdose, 7-2015, UpToDate, Vol. 2015, 2
M.L.A. Sivilotti, Management of Methanol and Ethylene Glycol Poisoning, 7-2015, UpToDate, Vol. 2015, 1
M.L.A. Sivilotti, Management of Isopropyl Alcohol Poisoning, 7-2015, UpToDate, Vol. 2015, 3
M.L.A. Sivilotti, Hematologic Principles, 6-2015, Goldfranks Toxicologic Emergencies, Vol. 22, 285-301
Editorials
Wong AY, Sivilotti ML, Dargan PI, Wood DM, Greene SL, Letter in reply to Riggan et al. Re: External validation of the paracetamol-aminotransferase multiplication product to predict hepatotoxicity from paracetamol overdose., 12-2015, Clinical toxicology (Philadelphia, Pa.), Vol. 53(10):1157
Wong A, Sivilotti ML, Dargan PI, Wood DM, Greene SL, Response to Letter to the Editor: External validation of the paracetamol-aminotransferase multiplication product to predict hepatotoxicity from paracetamol overdose., 12-2015, Clinical toxicology (Philadelphia, Pa.), Vol. 53(10):1154
Non-Peer-Reviewed Articles
Murray HE, Tiny Tips - Epinephrine Dosing, 11-2015, Boring EM
Murray HE, How to use likelihood ratios in everyday practice, 5-2015, Boring EM
Murray HE, Engaging students in research and critical appraisal, 3-2015, Boring EM
Murray HE, Mummydays: Balancing doctoring and mothering, 12-2015, CJEM, Vol. 7(6), 427-428
1. Mary Fran Hazinski, RN, MSN; Michael Shuster, MD; Michael W. Donnino, MD; Andrew H. Travers, MD, MSc; Ricardo A. Samson, MD; Steven M. Schexnayder, MD; Elizabeth H. Sinz, MD; Jeff A. Woodin, NREMT-, 2015 American Heart Association Guidelines for Emergency Cardiovascular Care and Cardiopulmonary Resuscitation: Highlights., 11-2015, American Heart Association
Dagnone JD, An accelerated path to competency-based education at Queens, 3-2015, Faculty of Health Sciences Deans Blog
Lew, J, Trebuss K, Moore, K, Six Steps to Reducing Ontario's Community Prescribed Opioid Load, 2-2015, Ontario Medical Review
Peer-Reviewed Abstracts
V Thiruganasambandamoorthy, M. Taljaard, I.G. Stiell, M. Sivilotti, M. Mukkaram, S. Kim, H. Murray, A. Vaidyanathan, B.H. Rowe, L.A. Calder, E. Lang, A. McRae, R. Sheldon, G.A. Wells, Emergency Department Management of Syncope - Need for Standardization and Improved Risk-Stratification, 6-2015, Can J Emerg Med, Vol. 17, S39-S40
V Thiruganasambandamoorthy, K. Kwong, M. Taljaard, M. Sivilotti, B.H. Rowe, R. Sheldon, G.A. Wells, I.G. Stiell., The Canadian Syncope Risk Score to Identify Patients at Risk for Serious Adverse Events after Emergency Department Disposition, 6-2015, Can J Emerg Med, Vol. 17, S6-S7
A. Wong, M.L. Sivilotti, P.I. Dargan, D.M. Wood, S.L. Greene, External validation of the paracetamol-aminotransferase multiplication product to predict hepatotoxicity from paracetamol overdose, 5-2015, Clin Toxicol, Vol. 53(4):353
V Thiruganasambandamoorthy, K. Kwong, M. Taljaard, M.L.A. Sivilotti, B.H. Rowe, R. Sheldon, G.A. Wells, I.G. Stiell., The Canadian Syncope Risk Score to Identify Patients at Risk for Serious Adverse Events after Emergency Department Disposition, 5-2015, Acad Emerg Med, Vol. 22(5 supp)
Y. Finkelstein, E.M. MacDonald, S. Hollands, J.R. Hutson, M.L.A. Sivilotti, M.M. Mamdani, G. Koren and D.N. Juurlink., Long-term Outcomes Following Deliberate Self-Poisoning in Teens: A Population-based Study, 4-2015, American Academy of Pediatrics, Vol. 2015, 1660.2
Y. Finkelstein, E.M. MacDonald, S. Hollands, J.R. Hutson, M.L. Sivilotti, M.M. Mamdani, G. Koren and D.N. Juurlink for the Canadian Drug Safety and Effectiveness Research Network, Long-term Outcomes Following Deliberate Self Poisoning: A Population-based Study, 3-2015, J Med Toxicol, Vol. 11, 2-3
Romolo Gaspari Srikar Adhikari Vicki Noble Jason Nomura Christopher Raio Daniel Theodoro Anthony Weekes Michael Woo Paul Atkinson David Blehar Samuel Brown Terrell Caffery Ashley Crimmins Samuel Lam M, Sonography in Cardiac Arrest: Real-time Assessment and Evaluation with Sonography Outcomes Network (REASON), 5-2015, Academic Emergency Medicine, Vol. 22, s1
R. Gaspari, MD, P.R. Atkinson, MD, M.Y. Woo, MD, L. Rang, MD, S. Adhikari, MD, V. Noble, MD, J. Nomura, MD, C. Raio, MD, D. Theodoro, MD, A. Weeks, MD, D. Blehar, MD, S. Brown, MD, T. Caffery, MD, A. , Sonography in cardiac arrest: Real-time Assessment and Evaluation with Sonography - Outcomes Network (REASON), 5-2015, CJEM, Vol. 17, s4
C. R. Bell, MD, C. McKaigney, MD, J. Newbigging, MD, M. Holden, MSc, L. Rang, MD, Ultrasound probe motion tracking as a novel tool for PoCUS competency assessment, 5-2015, CJEM, Vol. 17, s36
Justin Puntillo, Louise Rang, Rob Brison., Role of ED Ultasound in Diagnosing Dissection of Thoracic Aorta, 5-2015, CJEM, Vol. 17, s7
Katie Dainty and Steven C. Brooks, .A North American Survey of Public Opinion on the Acceptability of Crowdsourcing Basic Life Support for Out-of-hospital Cardiac Arrest, 3-2015, Circulation, Vol. 132, A19542
Derya Demirta, Steven C. Brooks, Laurie J. Morrison, and Timothy C. Y. Chan, Spatiotemporal Stability of Public Cardiac Arrests, 3-2015, Circulation, Vol. 132, A15003
Christopher Sun, Derya Demirtas, Steven C. Brooks, Laurie J. Morrison, Timothy Chan, Spatiotemporal AED location optimization, 4-2015, Circulation, Vol. 132, A16492
Christopher Sun, Derya Demirtas, Steven C. Brooks, Laurie J. Morrison, Timothy Chan, Ture Public Access Defibrillator Coverage is Overestimated, 3-2015, Circulation, Vol. 132, A15051
Tasha Hanuschak, Andrew Day, Paul Peng, Cathy Zahn, Laurie J. Morrison, and Steven C. Brooks, Coronary angiography after out-of-hospital cardiac arrest is associated with improved neurologically intact survival, 3-2015, Circulation, Vol. 132, A18724
Tasha Hanuschak, Andrew Day, Paul Peng, Cathy Zahn, Laurie J. Morrison, and Steven C. Brooks, Patient, Cardiac Arrest and Hospital Characteristics Associated With Receipt of Coronary Angiography in Out-of-Hospital Cardiac Arrest Patients, 4-2015, Circulation, Vol. 132, A18554
Hall AK, Dagnone JD, Sebok S, Moore S, Woolfrey K, Ross J, McNeil G, Hagel C, Davison C., Comparison of simulation-based resuscitation OSCE performance with ITER portfolio assessments of emergency medicine residents: A Canadian multi-center study, 7-2015, ICRE, Vol. 2015, 1
McGraw R, Keri Z, Chaplin T, Holden M, McKaigney C, Hall A, Rang L, Jaeger M, Messenger D, Redfearn D, Davison C, Fichtinger G, Ungi T, Yeo C., Development and evaluation of a simulation-based competency curriculum for ultrasound-guided central venous catheterization, 7-2015, ICRE, Vol. 87, 1
Bell CR, McKaigney C, Newbigging J, Holden M, Rang L, Ultrasound probe motion tracking as a novel tool for PoCUS competency assessment, 5-2015, Canadian Journal of Emergency Medicine, Vol. 17(S2):S36
L McLean, K Varette, K Baker, M Harvey, R Brison, A Day, women with less severe stress urinary incontinence symptoms are most likely to show a complete cure on a standardized pad test after performing a 12 week exercise program, 11-2015, Neurourology and Urodynamics, Vol. 34, s42-s43
Peer-Reviewed Articles
Pickett W, King N, Lawson J, Dosman JA, Trask C, Brison RJ, Hagel L, Janssen I, for the Saskatchewan Farm Injury Cohort Study Team, Farmers, mechanized work, and links to obesity., 1-2015, Preventive medicine, Vol. 70C, 59-63
Bruder EA, Ball I, Ridi S, Pickett W, Hohl C., Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients (Protocol), 1-2015, Cochrane Library, Vol. 1, N/A
Sibley S, Muscedere J, New-onset atrial fibrillation in critically ill patients., 12-2015, Canadian respiratory journal : journal of the Canadian Thoracic Society, Vol. 22(3):179-82
Redfearn DP Furqan MA, Enriquez A, Shaw C, Simpson C, Baranchuk A, Michael K, Abdollah H, Brison RJ, Emergency Department Re-Presentation for Atrial Fibrillation and Atrial Flutter, 8-2015, Canadian Journal of Cardiology, Vol. epub, epub ahead
Ting DK, Brison RJ, Injuries in recreational curling include head injuries and may be prevented by using proper footwear, 4-2015, Health Promotion and Chronic Disease Prevention in Canada, Vol. 35(2)
Wong JJ, CP, Ameis A, Varatharajan S, Varatharajan T, Shearer HM, Brison RJ, Sutton D, Randhawa K, Yu H, Southerst D, Goldgrub R, Mior S, Stupar M, Carroll LJ, Taylor-Vaisey A., Are non-steroidal anti-inflammatory drugs effective for the management of neck pain and associated disorders, whiplash-associated disorders, or non-specific low back pain? A systematic review of systematic reviews., 4-2015, Eur Spine J., Vol. 2015(4):1-28
Woitzik E, Jacobs C, Wong JJ, CP, Shearer HM, Randhawa K, Sutton D, Southerst D, Varatharajan S, Brison R, Yu H, van der Velde G, Stern PJ, Taylor-Vaisey A, Stupar M, Mior S, Carroll LJ., The effectiveness of exercise on recovery and clinical outcomes of soft tissue injuries of the leg, ankle, and foot: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration, 10-2015, Manual Therapy, Vol. 20(5):633-645
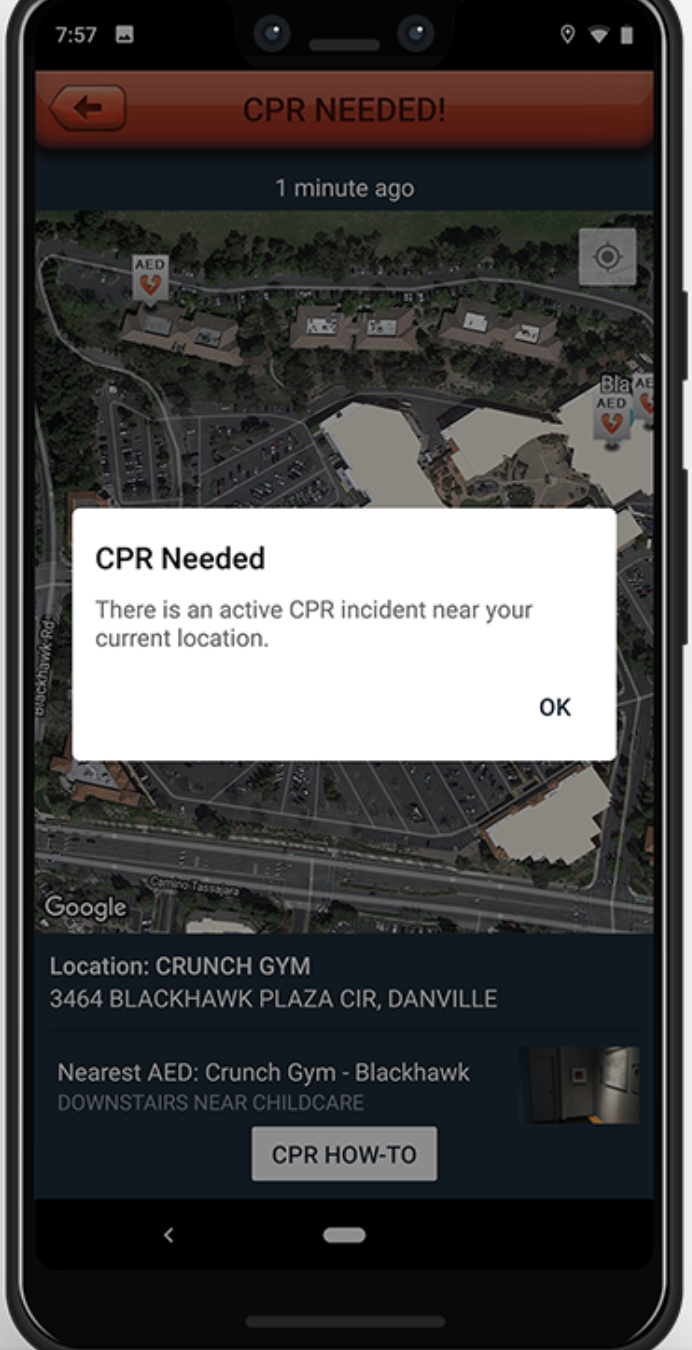
Steven C Brooks, Graydon Simmons, Heather Worthington, Bentley J Bobrow, Laurie J Morrison, The PulsePoint Respond mobile device application to crowdsource basic life support for patients with out-of-hospital cardiac arrest: Challenges for optimal implementation, 11-2015, Resuscitation, Vol. 98, 20-26
Steven C. Brooks; Monique L. Anderson; Eric Bruder ; Mohamud R. Daya; Alan Gaffney; Charles W. Otto; Adam J. Singer; Ravi R. Thiagarajan; Andrew H. Travers., Part 6: Alternative Techniques and Ancillary Devices for Cardiopulmonary Resuscitation, 10-2015, Circulation, Vol. 132, S436-S443
Clifton W. Callaway, Jasmeet Soar, Mayuki Aibiki; Bernd Bottiger; Steven C. Brooks; Charles Deakin; Michael W. Donnino; Saul Drajer; Walter Kloeck, Peter T. Morley; Laurie Morrison; Robert Neumar; Ton, Part 4: Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations, 10-2015, Circulation, Vol. 132, S84 - S145
Clifton W. Callaway, Jasmeet Soar, Mayuki Aibiki; Bernd Bottiger; Steven C. Brooks; Charles Deakin; Michael W. Donnino; Saul Drajer; Walter Kloeck, Peter T. Morley; Laurie Morrison; Robert Neumar; To, Part 4: Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations, 10-2015, Resuscitation, Vol. 95, e71-e120
Robert W. Neumar; Dianne L. Atkins; Farhan Bhanji; Steven C. Brooks; Clifton W. Callaway; Allan de Caen; Monica E. Kleinman; Steven L. Kronick; Eric J. Lavonas; Mark S. Link; Mary E. Mancini; Laurie M, Part 1: Executive Summary. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care., 10-2015, Circulation, Vol. 132, S315-S367
Farhan Bhanji, Judith C Finn, Andrew Lockey, Koenraad Monsieurs, Robert Frengley, Taku Iwami, Eddy Lang, Matthew Huei-Ming Ma, Mary E Mancini, Mary Ann McNeil, Robert Greif, John E Billi, Vinay M Nadk, Part 8: Education, Implementation, and Teams 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations, 9-2015, Circulation, Vol. 16(suppl 1):S242-S268
Mohamud R Daya; Robert H Schmicker; Dana Zive; Thomas D Rea; Graham Nichol; Jason E Buick; Steven Brooks; Jim Christenson; Renee MacPhee; Alan Craig; Jon C Rittenberger; Daniel P Davis; Susanne May; J, Out-of-Hospital Cardiac Arrest Survival Improving Over Time: Results from the Resuscitation Outcomes Consortium (ROC), 7-2015, Resuscitation, Vol. 91, 108-115
Ahamed H. Idris, Danielle Guffey, Paul P. Pepe, MD, Siobhan P. Brown, Steven C. Brooks, Clifton W. Callaway, Jim Christenson, Daniel P. Davis, Mohamud R. Daya, Randal Gray, Peter J. Kudenchuk, Jonatha, Chest compression rates and survival following out-of-hospital cardiac arrest, 4-2015, Critical Care Medicine, Vol. 43(4):840-848
Morrison LJ, Brooks SC, Dainty KN, Dorian P, Needham D, Ferguson ND, Rubenfeld GD, Slutsky AS, Wax RS, Zwarenstein M, Thorpe K, Zhan C, and Scales DC, on behalf of the Strategies for Post-Arrest Care , Improving the Use of Targeted Temperature Management After Out-of-Hospital Cardiac Arrest: A Stepped Wedge Cluster Randomized Trial., 5-2015, Critical Care Medicine, Vol. 43(5):954-964
Szulewski, A., Roth, N., & Howes, D., The Use of Task-Evoked Pupillary Response as an Objective Measure of Cognitive Load in Novices and Trained Physicians: A New Tool for the Assessment of Expertise, 7-2015, Academic Medicine, Vol. 90(7):981-987
Djogovic, D., MacDonald, S., Wensel, A., Green, R., Loubani, O., Archambault, P., Bordeleau, S., Messenger, D., Szulewski, A., Davidow, J., Kircher, J., Gray, S., Smith, K., Lee, J., Marc Benoit, J., Vasopressor and Inotrope Use in Canadian Emergency Departments: Evidence Based Consensus Guidelines., 7-2015, Canadian journal of emergency medicine, Vol. 17(Supp 1):1-16
Brooks SC, Anderson ML, Bruder E., Daya MR, Gaffney A, Otto CW, Singer AJ, Thiagarajan RR., Alternative Techniques and Ancillary Devices for Cardiopulmonary Resuscitation, 1-2015, American Heart Association, Vol. 132, N/A
Christopher Evans, Prehospital interventions for traumatic cardiac arrest: a systematic review - Dissertation, 9-2015, University of Oxford, Vol. xx, xx
Thiruganasambandamoorthy VI, Taljaard M, Stiell IG, Sivilotti ML, Murray HE, Vaidyanathan A, Rowe BH, Calder LA, Lang E, McRae A, Sheldon R, Wells GA, Emergency Department management of syncope: need for standardization and improved risk stratification., 4-2015, Internal Emergency Medicine, Vol. 10(5), 619-627
Trueger NS, Murray HE, Kobner S, Lin M., Global Emergency Medicine Journal Club: A Social Media Discussion About the Outpatient Management of Patients With Spontaneous Pneumothorax by Using Pigtail Catheters, 6-2015, Ann Emerg Medicine
Fernando SM, Cheskes S, Howes D, Hands-on defibrillation and electrocardiogram artefact filtering technology increases chest compression fraction and decreases peri-shock pause duration in a simulation model of cardiac arrest., 11-2015, CJEM
.K. Wasserman, J.J. Perry, D. Dowlatshahi, G. Stotts, M.L.A. Sivilotti, A. Worster, M. Emond, J. Sutherland, I. Stiell, M. Sharma, Isolated Transient Dysphasia at Emergency Presentation is Associated With a High Rate of Cardioembolic Embolism., 11-2015, Can J Emerg Med, Vol. 17(6):624-630
Finkelstein Y, Macdonald EM, Hollands S, Sivilotti ML, Hutson JR, Mamdani MM, Koren G, Juurlink DN, Canadian Drug Safety and Effectiveness Research Network (CDSERN), Risk of Suicide Following Deliberate Self-poisoning., 6-2015, JAMA Psychiatry, Vol. 72(6):570-5
Perry JJ, Alyahya B, Sivilotti ML, Bullard MJ, Emond M, Sutherland J, Worster A, Hohl C, Lee JS, Eisenhauer MA, Pauls M, Lesiuk H, Wells GA, Stiell IG, Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study., 2-2015, BMJ (Clinical research ed.), Vol. 350, h568
Hohl CM, Wickham ME, Sobolev B, Perry JJ, Sivilotti ML, Garrison S, Lang E, Brasher P, Doyle-Waters MM, Brar B, Rowe BH, Lexchin J, Holland R, The effect of early in-hospital medication review on health outcomes: a systematic review., 7-2015, British journal of clinical pharmacology, Vol. 80(1):51-61
Rowe BH, Singh M, Villa-Roel C, Leiter LA, Hramiak I, Edmonds ML, Lang E, Sivilotti M, Scheuermeyer F, Worster A, Riley J, Afilalo M, Stiell I, Yale JF, Woo VC, Campbell S, Canadian Association of Emergency Physicians Research Consortium., Acute management and outcomes of patients with diabetes mellitus presenting to Canadian emergency departments with hypoglycemia., 2-2015, Canadian journal of diabetes, Vol. 39(1):55-64
Thiruganasambandamoorthy V, Stiell IG, Sivilotti ML, Murray H, Rowe BH, Lang E, McRae A, Sheldon R, Wells GA, Risk stratification of adult emergency department syncope patients to predict short-term serious outcomes after discharge (RiSEDS) study., 3-2015, BMC emergency medicine, Vol. 14, 8
Finkelstein Y, Macdonald EM, Hollands S, Hutson JR, Sivilotti ML, Mamdani MM, Koren G, Juurlink DN, Canadian Drug Safety and Effectiveness Research Network (CDSERN), Long-term outcomes following self-poisoning in adolescents: a population-based cohort study., 6-2015, The lancet. Psychiatry, Vol. 2(6):532-9
Wong A, Sivilotti ML, Dargan PI, Wood DM, Greene SL, External validation of the paracetamol-aminotransferase multiplication product to predict hepatotoxicity from paracetamol overdose., 12-2015, Clinical toxicology (Philadelphia, Pa.), Vol. 53(8):807-14
M.J. Vermeulen, A. Guttmann, T.A. Stukel, A. Kachra, M.L.A. Sivilotti, B.H. Rowe, J. Dreyer, R. Bell, M. Schull, Are reductions in emergency department length of stay associated with improvements in quality of care? A difference-in-differences analysis, 8-2015, BMJ Qual Saf
Curtis RM, Sivilotti ML, A descriptive analysis of aspartate and alanine aminotransferase rise and fall following acetaminophen overdose., 11-2015, Clinical toxicology (Philadelphia, Pa.), Vol. 53(9):849-55
Sivilotti ML, Flumazenil, naloxone and the 'coma cocktail'., 8-2015, British journal of clinical pharmacology
Hagel CM, Hall AK, Dagnone JD, Queens University Emergency Medicine Simulation OSCE: an Advance in Competency-Based Assessment., 5-2015, Canadian Journal of Emergency Medicine, Vol. 20, 1-4
Hall AK, Dagnone JD, Lacroix LL, Pickett W, Klinger DA., Queens Simulation Assessment Tool (QSAT): Development and Validation of an Assessment Tool for Resuscitation OSCE Stations in Emergency Medicine, 4-2015, Simulation in Healthcare, Vol. 10(2):98-105
Hall AK, Dagnone JD, CAEP Feature Education Innovations (FEI): Competency-based Assessment of Resuscitation Skills by Simulation-based OSCE using the Queen?s Simulation Assessment Tool (QSAT)., 6-2015, CAEP Feature Education Innovations (FEI)
White M, Hall AK, What non-traditional learning methods are current emergency medicine (EM) residents using and to what extent do they find these resources beneficial compared to more traditional modalities?, 6-2015, CAEP Great Evidence in Medical Education (GEMeS)
Keri Z, Sydor D, Ungi T, Holden MS, McGraw R, Mousavi P, Borschneck DP, Fichtinger G, Jaeger M, Computerized training system for ultrasound-guided lumbar puncture on abnormal spine models: a randomized controlled trial., 7-2015, Canadian journal of anaesthesia = Journal canadien d'anesthesie, Vol. 62(7):777-84
Yeo CT, Davison C, Ungi T, Holden M, Fichtinger G, McGraw R, Examination of Learning Trajectories for Simulated Lumbar Puncture Training Using Hand Motion Analysis., 10-2015, Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, Vol. 22(10):1187-95
Clinkard D, Holden M, Ungi T, Messenger D, Davison C, Fichtinger G, McGraw R, The development and validation of hand motion analysis to evaluate competency in central line catheterization., 2-2015, Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, Vol. 22(2):212-8
Clinkard D, Moult E, Holden M, Davison C, Ungi T, Fichtinger G, McGraw R, Assessment of lumbar puncture skill in experts and nonexperts using checklists and quantitative tracking of needle trajectories: implications for competency-based medical education., 12-2015, Teaching and learning in medicine, Vol. 27(1):51-6
Dagnone JD, Simulation Olympics: innovations that showcase EM resident resuscitation skills., 6-2015, emsimcases.com
Hall AK, Dagnone JD, Lacroix L, Pickett W, Klinger DA, Queen's simulation assessment tool: development and validation of an assessment tool for resuscitation objective structured clinical examination stations in emergency medicine., 4-2015, Simulation in healthcare : journal of the Society for Simulation in Healthcare, Vol. 10(2):98-105
Wasserman JK, Perry JJ, Sivilotti ML, Sutherland J, Worster A, Emond M, Jin AY, Oczkowski WJ, Sahlas DJ, Murray H, MacKey A, Verreault S, Wells GA, Dowlatshahi D, Stotts G, Stiell IG, Sharma M, Computed tomography identifies patients at high risk for stroke after transient ischemic attack/nondisabling stroke: prospective, multicenter cohort study., 1-2015, Stroke; a journal of cerebral circulation, Vol. 46(1):114-9
Wong JJ, Shearer HM, Mior S, Jacobs C, Cote P, Randhawa K, Yu H, Southerst D, Varatharajan S, Sutton D, van der Velde G, Carroll LJ, Ameis A, Ammendolia C, Brison R, Nordin M, Stupar M, Taylor-Vaisey , Are manual therapies, passive physical modalities, or acupuncture effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? an update of the bone and joint decade task force on neck pain and its associated disorders by the optima collaboration., 12-2015, The spine journal : official journal of the North American Spine Society
Kleinman M.E., Brennan E, Goldberger Z.D., Swor R.A., Terry M, Bobrow B.J., Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality: American Heart Association Guidelines Update for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care, 1-2015, Circulation, Vol. 132, 414-35
Rouhani SA, Scott J, Greiner A, Albutt K, Hacker MR, Kuwert P, VanRooyen M, Bartels SA., Stigma and Parenting Children Conceived from Sexual Violence, 10-2015, American Academy of Pediatrics, Vol. 2015, 2014-3373
Becker T, Bartels SA, Hansoti J, Jacquet G, Lunney K, Marsh R, Osei-Ampofo M, Lam C, Levine A, Global Emergency Medicine: A review of the literature from 2014, 7-2015, Academic Emergency Medicine, Vol. epub, epub
Scott J, Rouhani S, Greiner A, Albutt K, Kuwert P, Hacker MR, VanRooyen M, Bartels S, Respondent-driven sampling to assess mental health outcomes, stigma and acceptance among women raising children born from sexual violence-related pregnancies in eastern Democratic Republic of Congo., 4-2015, BMJ open, Vol. 5(4):e007057
Wong H, Chen D, Moore K, Belanger P, Cunningham J, Peterson M., Analyzing Impact of Deer Habitat on the Spatial Dynamic of Lyme Risk in Eastern Ontario, 1-2015, Geo-Inf., Vol. 4(1), 105-12
Howes D, Gray SH, Brooks SC, Boyd JG, Djogovic D, Golan E, Green RS, Jacka MJ, Sinuff T, Chaplin T, Smith OM, Owen J, Szulewski A, Murphy L, Irvine S, Jichici D, Muscedere J, Canadian Guidelines for the use of targeted temperature management (therapeutic hypothermia) after cardiac arrest: A joint statement from The Canadian Critical Care Society (CCCS), Canadian Neurocritical Care Society (CNCCS), and the Canadian Critical Care Trials Group (CCCTG)., 9-2015, Resuscitation, Vol. 98, 48-63
Chaplin T, Archibald A, Kaul T, Howes D., A simulation-based trauma education program: does it improve trauma management?, 9-2015, MedEdPublish, Vol. 4, 14
Wood M, Song A, Maslove D, Ferri C, Howes D, Muscedere J, Boyd JG, Brain Tissue Oxygenation in Patients with Septic Shock: a Feasibility Study., 9-2015, The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques
Clinkard D, Cameron A, Howes D, Ball I, Targeted temperature management: It is not yet time to change your target temperature., 11-2015, CJEM, Vol. 17(6):706-8
Hall AK, Dagnone JD, Lacroix L, Pickett W, The development and validation of 10 simulation-based resuscitation OSCE stations for Emergency Medicine trainees, 4-2015, Simulation in Healthcare, Vol. 10(2):98-105
Dagnone JD, McGraw RM, Howes D, Messenger DK, Hall AK, Kaul T, Bruder E, Szulewski A, Chaplin T, OBrien T., How to Develop a Comprehensive Simulation-based Resuscitation Program in Emergency Medicine, 3-2015, Medical Teacher, Vol. 38(1):30-35
McKaigney, C., Diagnostic Challenge: A Ticklish belly button, 4-2015, Canadian Journal of Emergency Medicine, Vol. 22, 1-3
Pike I, Piedt S, Davison CM, Russell K, Macpherson AK, Pickett W, Youth injury prevention in Canada: use of the Delphi method to develop recommendations., 12-2015, BMC public health, Vol. 15(1):1274
Russell K, Davison C, King N, Pike I, Pickett W, Understanding clusters of risk factors across different environmental and social contexts for the prediction of injuries among Canadian youth., 11-2015, Injury
Elgar FJ, McKinnon B, Walsh SD, Freeman J, D Donnelly P, de Matos MG, Gariepy G, Aleman-Diaz AY, Pickett W, Molcho M, Currie C, Structural Determinants of Youth Bullying and Fighting in 79 Countries., 12-2015, The Journal of adolescent health : official publication of the Society for Adolescent Medicine, Vol. 57(6):643-50
Byrnes J, King N, Hawe P, Peters P, Pickett W, Davison C, Patterns of youth injury: a comparison across the northern territories and other parts of Canada., 12-2015, International journal of circumpolar health, Vol. 74, 27864
Vafaei A, Pickett W, Alvarado BE, Relationships between community social capital and injury in Canadian adolescents: a multilevel analysis, 12-2015, Injury prevention : journal of the International Society for Child and Adolescent Injury Prevention, Vol. 21(6):389-96
Dosman J, Hagel L, King N, Koehncke N, Kirychuk S, Trask C, Neudorf J, Day L, Voaklander D, Pickett W, Saskatchewan Farm Injury Cohort Study Team, The Hierarchy of Control in the Epidemic of Farm Injury., 12-2015, Journal of agromedicine, Vol. 20(3):360-9
DeWit Y, Pickett W, Lawson J, Dosman J, Saskatchewan Farm Injury Cohort Team, Farm Activities and Agricultural Injuries in Youth and Young Adult Workers., 12-2015, 1, Vol. 20(3):318-26
McMillan M, Trask C, Dosman J, Hagel L, Pickett W, Saskatchewan Farm Injury Cohort Study Team, Prevalence of Musculoskeletal Disorders Among Saskatchewan Farmers., 12-2015, Journal of agromedicine, Vol. 20(3):292-301
Chen Y, Rennie DC, Karunanayake CP, Janzen B, Hagel L, Pickett W, Dyck R, Lawson J, Dosman JA, Pahwa P, Saskatchewan Rural Health Study Group, Income adequacy and education associated with the prevalence of obesity in rural Saskatchewan, Canada., 7-2015, BMC public health, Vol. 15, 700
Pickett W, Elgar FJ, Reducing school violence in Africa: learning from Uganda., 7-2015, The Lancet. Global health, Vol. 3(7):e344-5
Tremblay MS, Gray C, Babcock S, Barnes J, Bradstreet CC, Carr D, Chabot G, Choquette L, Chorney D, Collyer C, Herrington S, Janson K, Janssen I, Larouche R, Pickett W, Power M, Sandseter EB, Simon B, , Position Statement on Active Outdoor Play., 6-2015, International journal of environmental research and public health, Vol. 12(6):6475-505
Gray C, Gibbons R, Larouche R, Sandseter EB, Bienenstock A, Brussoni M, Chabot G, Herrington S, Janssen I, Pickett W, Power M, Stanger N, Sampson M, Tremblay MS, What Is the Relationship between Outdoor Time and Physical Activity, Sedentary Behaviour, and Physical Fitness in Children? A Systematic Review., 6-2015, 1, Vol. 12(6):6455-74
Brussoni M, Gibbons R, Gray C, Ishikawa T, Sandseter EB, Bienenstock A, Chabot G, Fuselli P, Herrington S, Janssen I, Pickett W, Power M, Stanger N, Sampson M, Tremblay MS, What is the Relationship between Risky Outdoor Play and Health in Children? A Systematic Review., 6-2015, 2, Vol. 12(6):6423-54
Pickett W, Michaelson V, Davison C, Beyond nutrition: hunger and its impact on the health of young Canadians., 7-2015, International journal of public health, Vol. 60(5):527-38
Taylor-Gjevre RM, Trask C, King N, Koehncke N, Saskatchewan Farm Injury Cohort Study Team, Prevalence and occupational impact of arthritis in Saskatchewan farmers., 12-2015, Journal of agromedicine, Vol. 20(2):205-16
Pickett W, Ting N, Trask C, Michaelson V, Marlenga BL, Hagel L, Dosman JA, Saskatchewan Farm Injury Cohort Study Team, Factors Related to Self-perceived Health in Rural Men and Women., 12-2015, Journal of agromedicine, Vol. 20(2):178-87
Cozma I, Kukaswadia A, Janssen I, Craig W, Pickett W, Active transportation and bullying in Canadian schoolchildren: a cross-sectional study., 2-2015, BMC public health, Vol. 15, 99
Davison C, Michaelson V, Pickett W, It still takes a village: an epidemiological study of the role of social supports in understanding unexpected health states in young people., 3-2015, BMC public health, Vol. 15, 295
Looze Md, Raaijmakers Q, Bogt TT, Bendtsen P, Farhat T, Ferreira M, Godeau E, Kuntsche E, Molcho M, Pf�rtner TK, Simons-Morton B, Vieno A, Vollebergh W, Pickett W, Decreases in adolescent weekly alcohol use in Europe and North America: evidence from 28 countries from 2002 to 2010., 4-2015, European journal of public health, Vol. 25 Suppl 2, 69-72
Molcho M, Walsh S, Donnelly P, Matos MG, Pickett W, Trend in injury-related mortality and morbidity among adolescents across 30 countries from 2002 to 2010., 4-2015, 1, Vol. 25 Suppl 2, 33-6
Pulver A, Davison C, Pickett W, Time-use patterns and the recreational use of prescription medications among rural and small town youth., 12-2015, The Journal of rural health : official journal of the American Rural Health Association and the National Rural Health Care Association, Vol. 31(2):217-28
Janzen B, Karunanayake C, Pahwa P, Dyck R, Rennie D, Lawson J, Pickett W, Bryce R, Hagel L, Zhao G, Dosman J, Saskatchewan Rural Health Study Team, Exploring diversity in socioeconomic inequalities in health among rural dwelling Canadians., 12-2015, The Journal of rural health : official journal of the American Rural Health Association and the National Rural Health Care Association, Vol. 31(2):186-98
de Looze M, Janssen I, Elgar FJ, Craig W, Pickett W, Neighbourhood crime and adolescent cannabis use in Canadian adolescents., 1-2015, Drug and alcohol dependence, Vol. 146, 68-74
Michaelson V, Pickett W, Robinson P, Cameron L, Participation in church or religious groups and its association with health. Part 2: a qualitative, Canadian study., 6-2015, Journal of religion and health, Vol. 54(3):1118-33
Technical Reports
Blouin, Danielle, Blouin D. Residents perceptions of the positive and negative impacts of social interactions among residents and between residents and faculty on their learning., 11-2015, Medical Education conference
Eric Bruder, MD, FRCPC Heather White, MD Mark Froats, MD, FRCPC Rebecca Zur, MD Steve Brooks, MD, FRCPC, Potential Impact of an Early Extracorporeal Cardiopulmonary Resuscitation Strategy in Adult Cardiac Arrest, 6-2015, Canadian Association of Emergency Physicians